Treatment For Bursitis Of The Foot
Overview
Between the heel bone and the plantar fascia is a small fluid filled sac that is called the plantar (bottom of) calcaneal (heel bone) bursa. The plantar calcaneal bursa?s job is to allow the plantar fascia to glide easily over the heel bone without irritation. If this becomes inflamed and irritated a plantar calcaneal bursitis occurs which can be extremely painful and disabling forcing the athlete to stop training.
Causes
A rapid increase in physical activity levels or thinning of the heel?s protective fat pad are factors that may contribute to infracalcaneal bursitis. Other possible causes of infracalcaneal bursitis include blunt force trauma, acute or chronic infection, and arthritic conditions. The following factors may increase your risk of experiencing bursitis, including infracalcaneal bursitis. Participating in contact sports. Having a previous history of bursitis in any joint. Poor conditioning. Exposure to cold weather. Heel striking when running, especially in conventional running shoes with heel elevation.
Symptoms
Your feet are extremely resilient and are designed to stand up to the pressures of day-to-day living. In some cases, though, foot structures may break down when subjected to chronic stress associated with prolonged periods of weight-bearing activity on concrete, asphalt, or other hard surfaces (especially when your footwear does not allow for appropriate weight distribution). Foot problems, including infracalcaneal bursitis, are often exacerbated by poorly designed footwear, and pressure, impact, and shear forces can damage your feet over time. Bursal sacs are intended to minimize this damage, but sometimes the bursa itself becomes inflamed.
Diagnosis
If heel pain has not responded to home treatment, X-rays may be ordered. These images can show deformities of the heel bone and bone spurs that have developed at the attachment of the Achilles. If there is swelling and/or pain that is slightly higher and within the Achilles tendon itself, an MRI may be ordered to determine if the tendon is simply inflamed or if there is a chronic tear on the tendon. Aspiration and lab tests. If a septic bursitis is highly suspected, a doctor may perform an aspiration, removing fluid from the bursa with a needle and syringe. In addition to relieving pressure and making the patient more comfortable, it provides a fluid sample that can be tested for infection.
Non Surgical Treatment
Conservative treatment of bursitis is usually effective. The application of heat, rest, and immobilization of the affected joint area is the first step. A sling can be used for a shoulder injury, a cane is helpful for hip problems. The patient can take nonsteroidal anti-inflammatory drugs (NSAIDs) like aspirin, ibuprofin, and naproxen. They can be obtained without a prescription and relieve the pain and inflammation. Once the pain decreases, exercises of the affected area can begin. If the nearby muscles have become weak because of the disease or prolonged immobility, then exercises to build strength and improve movement are best. A doctor or physical therapist can prescribe an effective regimen. If the bursitis is related to an inflammatory condition like arthritis or gout, then management of that disease is needed to control the bursitis. When bursitis does not respond to conservative treatment, an injection into the joint of a long-acting corticosteroid preparation, like prednisone, can bring immediate and lasting relief. A corticosteroid is a hormonal substance that is the most effective drug for reducing inflammation. The drug is mixed with a local anesthetic and works on the joint within five minutes. Usually one injection is all that is needed.
Surgical Treatment
Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).
Prevention
You may be able to prevent bursitis from happening or coming back. Continue your home treatment with rest, ice, pain relievers, and gentle exercises. When you are ready to try the activity that caused the pain, start slowly and do it for short periods or at a slower speed. Warm up before and stretch after the activity. Increase your activity slowly, and stop if it hurts. Use ice afterward to prevent pain and swelling. Change the way you do activities with repeated movements that may strain your muscles or joints. For example if using a certain tool has caused bursitis, start switching hands or change the grip size of your tool. If sitting for long periods has caused bursitis, get up and walk around every hour. If a certain sport is causing bursitis, consider taking lessons to learn proper techniques. Have an expert check your equipment to make sure it's well suited to your size, strength, and ability. If certain activities at work may be causing bursitis, talk to your human resources department about other ways of doing your job, equipment changes, or other job assignments. Protect your joints from pressure. Cushion knees or elbows on hard surfaces, and wear shoes that fit you well and have good support.
Between the heel bone and the plantar fascia is a small fluid filled sac that is called the plantar (bottom of) calcaneal (heel bone) bursa. The plantar calcaneal bursa?s job is to allow the plantar fascia to glide easily over the heel bone without irritation. If this becomes inflamed and irritated a plantar calcaneal bursitis occurs which can be extremely painful and disabling forcing the athlete to stop training.
Causes
A rapid increase in physical activity levels or thinning of the heel?s protective fat pad are factors that may contribute to infracalcaneal bursitis. Other possible causes of infracalcaneal bursitis include blunt force trauma, acute or chronic infection, and arthritic conditions. The following factors may increase your risk of experiencing bursitis, including infracalcaneal bursitis. Participating in contact sports. Having a previous history of bursitis in any joint. Poor conditioning. Exposure to cold weather. Heel striking when running, especially in conventional running shoes with heel elevation.
Symptoms
Your feet are extremely resilient and are designed to stand up to the pressures of day-to-day living. In some cases, though, foot structures may break down when subjected to chronic stress associated with prolonged periods of weight-bearing activity on concrete, asphalt, or other hard surfaces (especially when your footwear does not allow for appropriate weight distribution). Foot problems, including infracalcaneal bursitis, are often exacerbated by poorly designed footwear, and pressure, impact, and shear forces can damage your feet over time. Bursal sacs are intended to minimize this damage, but sometimes the bursa itself becomes inflamed.
Diagnosis
If heel pain has not responded to home treatment, X-rays may be ordered. These images can show deformities of the heel bone and bone spurs that have developed at the attachment of the Achilles. If there is swelling and/or pain that is slightly higher and within the Achilles tendon itself, an MRI may be ordered to determine if the tendon is simply inflamed or if there is a chronic tear on the tendon. Aspiration and lab tests. If a septic bursitis is highly suspected, a doctor may perform an aspiration, removing fluid from the bursa with a needle and syringe. In addition to relieving pressure and making the patient more comfortable, it provides a fluid sample that can be tested for infection.
Non Surgical Treatment
Conservative treatment of bursitis is usually effective. The application of heat, rest, and immobilization of the affected joint area is the first step. A sling can be used for a shoulder injury, a cane is helpful for hip problems. The patient can take nonsteroidal anti-inflammatory drugs (NSAIDs) like aspirin, ibuprofin, and naproxen. They can be obtained without a prescription and relieve the pain and inflammation. Once the pain decreases, exercises of the affected area can begin. If the nearby muscles have become weak because of the disease or prolonged immobility, then exercises to build strength and improve movement are best. A doctor or physical therapist can prescribe an effective regimen. If the bursitis is related to an inflammatory condition like arthritis or gout, then management of that disease is needed to control the bursitis. When bursitis does not respond to conservative treatment, an injection into the joint of a long-acting corticosteroid preparation, like prednisone, can bring immediate and lasting relief. A corticosteroid is a hormonal substance that is the most effective drug for reducing inflammation. The drug is mixed with a local anesthetic and works on the joint within five minutes. Usually one injection is all that is needed.
Surgical Treatment
Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).
Prevention
You may be able to prevent bursitis from happening or coming back. Continue your home treatment with rest, ice, pain relievers, and gentle exercises. When you are ready to try the activity that caused the pain, start slowly and do it for short periods or at a slower speed. Warm up before and stretch after the activity. Increase your activity slowly, and stop if it hurts. Use ice afterward to prevent pain and swelling. Change the way you do activities with repeated movements that may strain your muscles or joints. For example if using a certain tool has caused bursitis, start switching hands or change the grip size of your tool. If sitting for long periods has caused bursitis, get up and walk around every hour. If a certain sport is causing bursitis, consider taking lessons to learn proper techniques. Have an expert check your equipment to make sure it's well suited to your size, strength, and ability. If certain activities at work may be causing bursitis, talk to your human resources department about other ways of doing your job, equipment changes, or other job assignments. Protect your joints from pressure. Cushion knees or elbows on hard surfaces, and wear shoes that fit you well and have good support.
Hammer Toe Disorder
 Overview
Overview
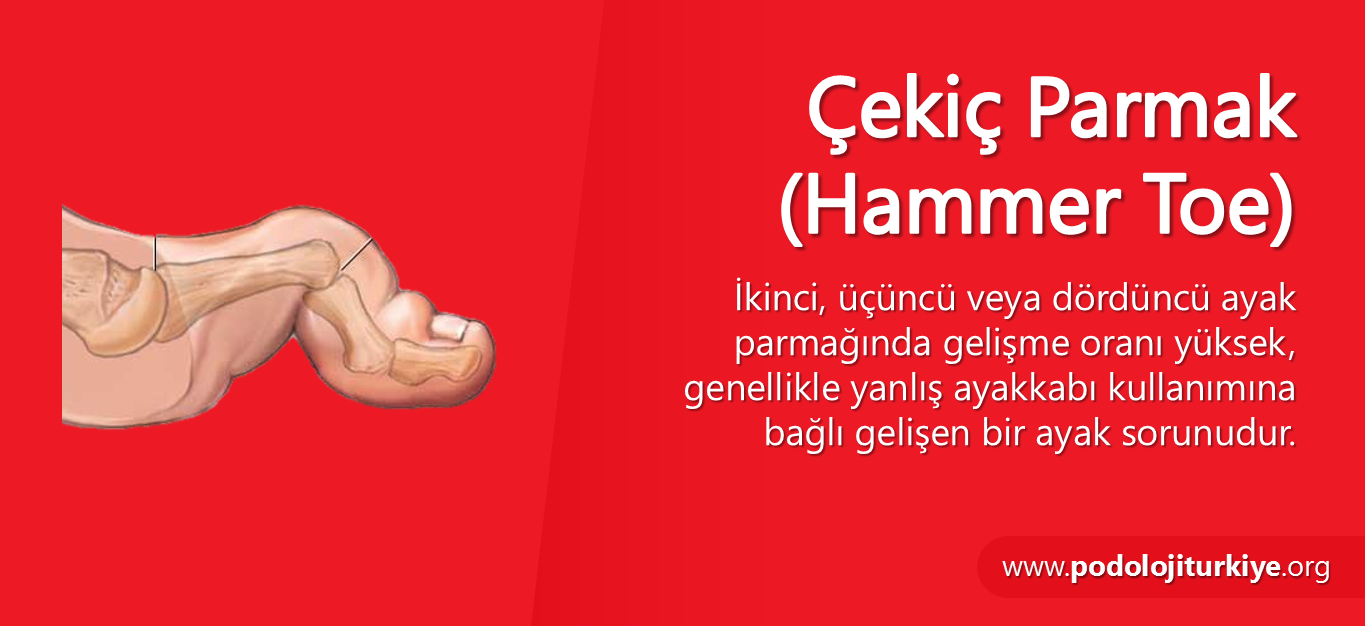
Hammer, claw, and mallet toes are toes that do not have the right shape. They may look odd or may hurt, or both. Tight shoes are the most common cause of these toe problems. A Hammer toes is a toe that bends down toward the floor at the middle toe joint. It usually happens in the second toe. This causes the middle toe joint to rise up. Hammer toes often occur with bunions. Claw toe often happens in the four smaller toes at the same time. The toes bend up at the joints where the toes and the foot meet. They bend down at both the middle joints and at the joints nearest the tip of the toes. This causes the toes to curl down toward the floor. A mallet toe often happens to the second toe, but it may happen in the other toes as well. The toe bends down at the joint closest to the tip of the toe.
Causes
Hammertoes are most common in women, and a big part of this is poor shoe choices, which are a big factor in the development of many foot problems. Tight toe boxes and high heels are the biggest culprits. Genetics certainly plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. But most cases of contracted toes are associated with various biomechanical abnormalities in how a patient walks. This causes the muscles and tendons to be used excessively or improperly, which deforms the toes over time.
 Symptoms
Symptoms
Hammer toe is often distinguished by a toe stuck in an upside-down ?V? position, and common symptoms include corns on the top of your toe joint. Pain at the top of a bent toe when you put on your shoes. Pain when moving a toe joint. Pain on the ball of your foot under the bent toe. Corns developing on the top of the toe joint. It is advisable to seek medical advice if your feet hurt on a regular basis. It is imperative to act fast and seek the care of a podiatrist or foot surgeon. By acting quickly, you can prevent your problem from getting worse.
Diagnosis
The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Non Surgical Treatment
Pad it. Mild cases of hammertoe can be treated with corn pads or felt pads available in the pharmacy. Toe Hammer toe caps, the small, padded sleeves that fit around the tip of the toe, may relieve hammer toe pain. Change your shoes. Wear wide shoes with resilient soles. Avoid shoes with pointed toes. Exercise. Certain exercises such as moving and stretching your toe gently with your hands and picking small or soft objects such as marbles or towels can keep your toe joints flexible. Also, while you are watching television or reading, you can also put a towel flat under your feet and use your toes to crumple it. This simple exercise can stretch and strengthen your muscles. Use ice. If your hammer toe becomes painful, applying an ice pack several times a day can help relieve the soreness and swelling.
Take medications. Nonsteroidal anti-inflammatory medicines (also called NSAIDs), such as ibuprofen or naproxen may be helpful in minimizing pain and inflammation. Use orthotic devices. Place a custom orthotic device in your shoe. This will help control the muscle/tendon imbalance.
Surgical Treatment
If a person's toes have become very inflexible and unresponsive to non-invasive means of treatment and if open sores have developed as a result of constant friction, they may receive orthopaedic surgery to correct the deformity. The operation is quick and is commonly performed as an out-patient procedure. The doctor administers a local anesthetic into the person's foot to numb the site of the operation. The person may remain conscious as the surgeon performs the procedure. A sedative might also be administered to help calm the person if they are too anxious.
What Are The Treatments For Bunions?
Overview
 The term hallux valgus actually describes what happens to the big toe. Hallux is the medical term for big toe, and valgus is an anatomic term that means the deformity goes in a direction away from the midline of the body. So in hallux valgus the big toe begins to point towards the outside of the foot. As this condition worsens, other changes occur in the foot that increase the problem. One of those changes is that the bone just above the big toe, the first metatarsal, usually develops too much of an angle in the other direction. This condition is called metatarsus primus varus. Metatarsus primus means first metatarsal, and varus is the medical term that means the deformity goes in a direction towards the midline of the body. This creates a situation where the first metatarsal and the big toe now form an angle with the point sticking out at the inside edge of the ball of the foot. The bunion that develops is actually a response to the pressure from the shoe on the point of this angle. At first the bump is made up of irritated, swollen tissue that is constantly caught between the shoe and the bone beneath the skin. As time goes on, the constant pressure may cause the bone to thicken as well, creating an even larger lump to rub against the shoe.
The term hallux valgus actually describes what happens to the big toe. Hallux is the medical term for big toe, and valgus is an anatomic term that means the deformity goes in a direction away from the midline of the body. So in hallux valgus the big toe begins to point towards the outside of the foot. As this condition worsens, other changes occur in the foot that increase the problem. One of those changes is that the bone just above the big toe, the first metatarsal, usually develops too much of an angle in the other direction. This condition is called metatarsus primus varus. Metatarsus primus means first metatarsal, and varus is the medical term that means the deformity goes in a direction towards the midline of the body. This creates a situation where the first metatarsal and the big toe now form an angle with the point sticking out at the inside edge of the ball of the foot. The bunion that develops is actually a response to the pressure from the shoe on the point of this angle. At first the bump is made up of irritated, swollen tissue that is constantly caught between the shoe and the bone beneath the skin. As time goes on, the constant pressure may cause the bone to thicken as well, creating an even larger lump to rub against the shoe.
Causes
Bunions result from the long bone in the foot (metatarsal) and the big-toe bone becoming misaligned. The causes are likely to be a combination of genetics, wearing ill-fitting shoes, and the way that we walk or run. Arthritis sufferers are also prone to bunions.
Symptoms
Bunions may or may not cause symptoms. A frequent symptom is foot pain in the involved area when walking or wearing shoes that is relieved by resting. A bunion causes enlargement of the base of the big toe and is usually associated with positioning of the big toe toward the smaller toes. This leads to intermittent or chronic pain at the base of the big toe. Bunions that cause marked pain are often associated with swelling of the soft tissues, redness, and local tenderness. It is important to note that, in post-pubertal men and post-menopausal women, pain at the base of the big toe can be caused by gout and gouty arthritis that is similar to the pain caused by bunions.
Diagnosis
Your family doctor or chiropodist /podiatrist can identify a bunion simply by examining your foot. During the exam, your big toe will be moved up and down to determine if your range of motion is limited. You will be examined for signs of redness or swelling and be questioned about your history of pain. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen. A X-ray of your foot may help identify the cause of the bunion and rate its severity.
Non Surgical Treatment
Sometimes observation of the bunion is all that?s needed. To reduce the chance of damage to the joint, periodic evaluation and x-rays by your surgeon are advised. In many other cases, however, some type of treatment is needed. Early treatments are aimed at easing the pain of bunions, but they won?t reverse the deformity itself. These include changes in shoewear. Wearing the right kind of shoes is very important. Choose shoes that have a wide toe box and forgo those with pointed toes or high heels which may aggravate the condition. Padding. Pads placed over the area of the bunion can help minimize pain. These can be obtained from your surgeon or purchased at a drug store. Activity modifications. Avoid activity that causes bunion pain, including standing for long periods of time. Medications. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Icing. Applying an ice pack several times a day helps reduce inflammation and pain. Injection therapy. Although rarely used in bunion treatment, injections of corticosteroids may be useful in treating the inflamed bursa (fluid-filled sac located around a joint) sometimes seen with bunions. Orthotic devices. In some cases, custom orthotic devices may be provided by the foot and ankle surgeon. 
Surgical Treatment
If nonsurgical treatment fails, you may want to consider surgery. Many studies have found that 85 to 90 percent of patients who undergo bunion surgery are satisfied with the results. Reasons that you may benefit from bunion surgery commonly include severe foot pain that limits your everyday activities, including walking and wearing reasonable shoes. You may find it hard to walk more than a few blocks (even in athletic shoes) without significant pain. Chronic big toe inflammation and swelling that doesn't improve with rest or medications. Toe deformity-a drifting in of your big toe toward the small toes. Toe stiffness-inability to bend and straighten your toe. Failure to obtain pain relief from nonsteroidal anti-inflammatory drugs. Their effectiveness in controlling toe pain varies greatly from person to person. Failure to substantially improve with other treatments such as a change in shoes and anti-inflammatory medication. As you explore bunion surgery, be aware that so-called "simple" or "minimal" surgical procedures are often inadequate "quick fixes" that can do more harm than good. And beware of unrealistic claims that surgery can give you a "perfect" foot. The goal of surgery is to relieve as much pain, and correct as much deformity as is realistically possible. It is not meant to be cosmetic.
Do I Suffer From Over-Pronation
Overview
When standing, pronation occurs as the foot rolls inwards and the arch of the foot flattens. Pronation is a normal part of the gait cycle which helps to provide shock absorption at the foot. The opposite movement to pronation is supination. This is also a normal part of the gait cycle just after the heel strike however over-supination is also not good.
Causes
Congenital "Flat Feet" - an individual may be born with feet that lack an appropriately supportive arch thereby predisposing the individual to this foot condition. Excessive Weight (Obesity) Too much weight on the foot from either obesity or pregnancy may be a factor. Repetitive Impact walking on flat, hard surfaces continuously places unnatural stress on the foot arch.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Prevention
Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot.
When standing, pronation occurs as the foot rolls inwards and the arch of the foot flattens. Pronation is a normal part of the gait cycle which helps to provide shock absorption at the foot. The opposite movement to pronation is supination. This is also a normal part of the gait cycle just after the heel strike however over-supination is also not good.
Causes
Congenital "Flat Feet" - an individual may be born with feet that lack an appropriately supportive arch thereby predisposing the individual to this foot condition. Excessive Weight (Obesity) Too much weight on the foot from either obesity or pregnancy may be a factor. Repetitive Impact walking on flat, hard surfaces continuously places unnatural stress on the foot arch.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Prevention
Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot.
Severs Disease The Facts
Overview
A syndrome of heel pain in skeletally immature individuals. The formal name is: calcaneal apophysitis. The pain is thought to arise from the growth plate (apophysis) and epiphysis. It is thought to be an overuse phenomena. Overloading of the apophysis by both traction (due to Achilles tendon) and compression (sue to weightbearing) have been implicated. Reversible pathologic alterations occur in the apophysis, which cause secondary pain. It is the growth plate and its bone, at the back of the heel bone (calcaneus), whose presence allows for longitudinal growth of calcaneus.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
The most common symptoms of Sever?s involves pain or tenderness in one or both heels. This pain usually occurs at the back of the heel, but can also extend to the sides and bottom of the heel. A child with Sever?s may also have these common problems, Heel pain with limping, especially after running. Difficulty walking, Discomfort or stiffness in the feet upon awaking. Swelling and redness in the heel, Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
There is nothing you can do to stop severs disease. It will stop when you finish growing. However the following will help to relieve the symptoms. Rest. Cut down on the time you spend playing sport until the pain has gone. Avoid sports that involve a lot of running or jumping. Swimming can be a useful alternative. Ice the affected area for ten to 15 minutes, especially after activity. Make sure you protect the skin by wrapping the ice in a towel. Elevate (raise) the leg when painful and swollen especially after sports. Pain relieving medication may reduce pain and swelling, but you need to discuss options with a pharmacist or GP. Always wear shoes. Avoid activities in bare feet. Choose a supportive shoe with the laces done up.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
A syndrome of heel pain in skeletally immature individuals. The formal name is: calcaneal apophysitis. The pain is thought to arise from the growth plate (apophysis) and epiphysis. It is thought to be an overuse phenomena. Overloading of the apophysis by both traction (due to Achilles tendon) and compression (sue to weightbearing) have been implicated. Reversible pathologic alterations occur in the apophysis, which cause secondary pain. It is the growth plate and its bone, at the back of the heel bone (calcaneus), whose presence allows for longitudinal growth of calcaneus.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
The most common symptoms of Sever?s involves pain or tenderness in one or both heels. This pain usually occurs at the back of the heel, but can also extend to the sides and bottom of the heel. A child with Sever?s may also have these common problems, Heel pain with limping, especially after running. Difficulty walking, Discomfort or stiffness in the feet upon awaking. Swelling and redness in the heel, Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
There is nothing you can do to stop severs disease. It will stop when you finish growing. However the following will help to relieve the symptoms. Rest. Cut down on the time you spend playing sport until the pain has gone. Avoid sports that involve a lot of running or jumping. Swimming can be a useful alternative. Ice the affected area for ten to 15 minutes, especially after activity. Make sure you protect the skin by wrapping the ice in a towel. Elevate (raise) the leg when painful and swollen especially after sports. Pain relieving medication may reduce pain and swelling, but you need to discuss options with a pharmacist or GP. Always wear shoes. Avoid activities in bare feet. Choose a supportive shoe with the laces done up.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Posterior Tibial Tendon Dysfunction Orthotic Treatment
Overview
Originally known as posterior tibial tendon dysfunction or insufficiency, adult-acquired flatfoot deformity encompasses a wide range of deformities. These deformities vary in location, severity, and rate of progression. Establishing a diagnosis as early as possible is one of the most important factors in treatment. Prompt early, aggressive nonsurgical management is important. A patient in whom such treatment fails should strongly consider surgical correction to avoid worsening of the deformity. In all four stages of deformity, the goal of surgery is to achieve proper alignment and maintain as much flexibility as possible in the foot and ankle complex. However, controversy remains as to how to manage flexible deformities, especially those that are severe. 
Causes
There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction.
Symptoms
Pain and swelling behind the inside of your ankle and along your instep. You may be tender behind the inner ankle where the posterior tibial tendon courses and occasionally get burning, shooting, tingling or stabbing pain as a result of inflammation of the nerve inside the tarsal tunnel. Difficulty walking, the inability to walk long distances and a generalised ache while walking even short distances. This may probably become more pronounced at the end of each day. Change in foot shape, sometimes your tendon stretches out, this is due to weakening of the tendon and ligaments. When this occurs, the arch in your foot flattens and a flatfoot deformity occurs, presenting a change in foot shape. Inability to tip-toe, a way of diagnosing Posterior Tibial Tendon Dysfunction is difficulty or inability to ?heel rise? (stand on your toes on one foot). Your tibialis posterior tendon enables you to perform this manoeuvre effectively. You may also experience pain upon attempting to perform a heel rise.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
Nonoperative therapy for posterior tibial tendon dysfunction has been shown to yield 67% good-to-excellent results in 49 patients with stage 2 and 3 deformities. A rigid UCBL orthosis with a medial forefoot post was used in nonobese patients with flexible heel deformities correctible to neutral and less than 10? of forefoot varus. A molded ankle foot orthosis was used in obese patients with fixed deformity and forefoot varus greater than 10?. Average length of orthotic use was 15 months. Four patients ultimately elected to have surgery. The authors concluded that orthotic management is successful in older low-demand patients and that surgical treatment can be reserved for those patients who fail nonoperative treatment. 
Surgical Treatment
Surgery is usually performed when non-surgical measures have failed. The goal of surgery is to eliminate pain, stop progression of the deformity and improve a patient?s mobility. More than one technique may be used, and surgery tends to include one or more of the following. The tendon is reconstructed or replaced using another tendon in the foot or ankle The name of the technique depends on the tendon used. Flexor digitorum longus (FDL) transfer. Flexor hallucis longus (FHL) transfer. Tibialis anterior transfer (Cobb procedure). Calcaneal osteotomy - the heel bone may be shifted to bring your heel back under your leg and the position fixed with a screw. Lengthening of the Achilles tendon if it is particularly tight. Repair one of the ligaments under your foot. If you smoke, your surgeon may refuse to operate unless you can refrain from smoking before and during the healing phase of your procedure. Research has proven that smoking delays bone healing significantly.
Heel And Arch Pain Causes
Overview
If you are dealing with chronic pain in the arch of your foot (the area between the ball and heel) it may be diagnosed as arch strain. While there are several potential causes for arch pain, the most common cause is plantar fasciitis. The plantar fascia is the band of ligaments that runs along the sole of the foot, connecting the heel bone to the metatarsals (bones just behind the toes.) Its job is to support the arch of your foot, and to put some ?spring in your step.? But, unfortunately, it?s the sight of an all-to-common inflammation that causes intense pain in the heel and across the bottom of the foot. This inflammation and pain is known as plantar fasciitis.

Causes
There are many different causes of flat feet, which can be separated into two main categories. The first category, congenital flat foot, is a condition that one is born with or is predisposed to at birth. This type includes the completely asymptomatic, pediatric flexible flat foot-by far the most common form of congenital flat foot. Flexible means that an arch is present until weight is put on the foot, at which time the arch disappears. This foot type is a result of the fact that all people are born with different physical features. Some people have bigger noses than others, just as some people have flatter feet (of course, there is no known correlation between the two). Any alteration in the many building blocks of the foot can influence its shape.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused. If you notice that the twinges of pain you have are most commonly associated with or immediately after exercise, you might want to visit a good athletic shoe store to make sure you are wearing the right kind of shoe. Another cause of arch pain is plantar fasciitis. The plantar fascia is a tough tissue structure that holds the bottom part of the arch in place. The fascia often becomes inflamed and sore, usually as a result of repetitive motion (for example, very common in those who stand on their feet for work). The pain is often noticeable first thing in the morning and worse with activity.
Diagnosis
In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics.
Non Surgical Treatment
In mild cases patients would benefit from custom made semi rigid full length custom made foot orthoses fitted into appropriate supportive footwear, preferably with laces or a velcro straps. In more severe cases patients may require a custom made Arizona lace up ankle brace or a posterior shell Ankle Foot Orthosis. These offer significantly more control and support than the foot orthoses. In severe cases surgery may be required to repair the tibialis posterior tendon and realign the foot and ankle, or fuse the subtalar joint. It is important to note there are many risks involved in having surgery and these must be considered prior to going ahead.

Surgical Treatment
As with most surgeries, patients and physicians should consider the surgery only after other, less invasive treatments have proven unproductive. Indications for surgery include Pain. Inability to function. Failure to improve after a six-month course of specific, directed physical therapy. Failure to improve after using arch supports, orthotics, or ankle and foot bracing. Once patients are at that point, the good news is that the procedure has considerably better outcomes than more traditional flat foot surgery. In the past, surgeons would realign and fuse the three hind joints, which would cause patients to lose motion, leaving them with a significantly stiff hind foot, With these newer procedures, if the foot is still flexible, surgeons can realign it and usually restore a close-to-normal or functional range of motion in the joints.
Prevention
Maintain a healthy weight, Use insoles to support your arches, Limit how often you wear high heels, Use proper shoes, especially when exercising to evenly distribute weight through your foot.
Stretching Exercises
Strength training and stretching can help avoid injury and keep your feet free from pain. Stretching should focus on the bottom of your foot to loosen tissues and tight ligaments surrounding your arch. The easiest way to do this is by grabbing a towel and sitting on the floor. You can do this while you catch up on the news in the morning, or when you get home from work. Put one leg out in front with your foot flexed up. Loop the towel around the ball of your foot and gently pull your toes towards you. Hold for thirty seconds and then repeat 3-4 times before switching feet.
If you are dealing with chronic pain in the arch of your foot (the area between the ball and heel) it may be diagnosed as arch strain. While there are several potential causes for arch pain, the most common cause is plantar fasciitis. The plantar fascia is the band of ligaments that runs along the sole of the foot, connecting the heel bone to the metatarsals (bones just behind the toes.) Its job is to support the arch of your foot, and to put some ?spring in your step.? But, unfortunately, it?s the sight of an all-to-common inflammation that causes intense pain in the heel and across the bottom of the foot. This inflammation and pain is known as plantar fasciitis.
Causes
There are many different causes of flat feet, which can be separated into two main categories. The first category, congenital flat foot, is a condition that one is born with or is predisposed to at birth. This type includes the completely asymptomatic, pediatric flexible flat foot-by far the most common form of congenital flat foot. Flexible means that an arch is present until weight is put on the foot, at which time the arch disappears. This foot type is a result of the fact that all people are born with different physical features. Some people have bigger noses than others, just as some people have flatter feet (of course, there is no known correlation between the two). Any alteration in the many building blocks of the foot can influence its shape.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused. If you notice that the twinges of pain you have are most commonly associated with or immediately after exercise, you might want to visit a good athletic shoe store to make sure you are wearing the right kind of shoe. Another cause of arch pain is plantar fasciitis. The plantar fascia is a tough tissue structure that holds the bottom part of the arch in place. The fascia often becomes inflamed and sore, usually as a result of repetitive motion (for example, very common in those who stand on their feet for work). The pain is often noticeable first thing in the morning and worse with activity.
Diagnosis
In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics.
Non Surgical Treatment
In mild cases patients would benefit from custom made semi rigid full length custom made foot orthoses fitted into appropriate supportive footwear, preferably with laces or a velcro straps. In more severe cases patients may require a custom made Arizona lace up ankle brace or a posterior shell Ankle Foot Orthosis. These offer significantly more control and support than the foot orthoses. In severe cases surgery may be required to repair the tibialis posterior tendon and realign the foot and ankle, or fuse the subtalar joint. It is important to note there are many risks involved in having surgery and these must be considered prior to going ahead.
Surgical Treatment
As with most surgeries, patients and physicians should consider the surgery only after other, less invasive treatments have proven unproductive. Indications for surgery include Pain. Inability to function. Failure to improve after a six-month course of specific, directed physical therapy. Failure to improve after using arch supports, orthotics, or ankle and foot bracing. Once patients are at that point, the good news is that the procedure has considerably better outcomes than more traditional flat foot surgery. In the past, surgeons would realign and fuse the three hind joints, which would cause patients to lose motion, leaving them with a significantly stiff hind foot, With these newer procedures, if the foot is still flexible, surgeons can realign it and usually restore a close-to-normal or functional range of motion in the joints.
Prevention
Maintain a healthy weight, Use insoles to support your arches, Limit how often you wear high heels, Use proper shoes, especially when exercising to evenly distribute weight through your foot.
Stretching Exercises
Strength training and stretching can help avoid injury and keep your feet free from pain. Stretching should focus on the bottom of your foot to loosen tissues and tight ligaments surrounding your arch. The easiest way to do this is by grabbing a towel and sitting on the floor. You can do this while you catch up on the news in the morning, or when you get home from work. Put one leg out in front with your foot flexed up. Loop the towel around the ball of your foot and gently pull your toes towards you. Hold for thirty seconds and then repeat 3-4 times before switching feet.